Why ERP? A Look Into the Gold Standard Treatment for OCD
Exposure and Response-Prevention (ERP) is widely known as the “Gold Standard” therapy for Obsessive-Compulsive Disorder. There is an incredibly wide body of evidence that supports ERP’s effectiveness for OCD, including that it it is certainly more effective than SSRI medication treatment alone. More and more folks who struggle with OCD are learning that traditional “talk therapy” is generally ineffective when it comes to treating OCD and helping them stop engaging in compulsions. But why is ERP a better choice? What does it involve? How is it different from regular talk therapy? These are all questions I’m excited to answer, but first let’s review some basic info about OCD.
The OCD Cycle
OCD is a specific anxiety disorder that typically involves obsessions/intrusive thoughts that fall within a particular “theme”; these thoughts are frequent and consume a significant amount (1hr per day or more) of a person’s time. The person with OCD interprets these thoughts as incredibly distressing, and then engages in specific behaviors (compulsions) with the intention of neutralizing the thoughts and the uncomfortable feelings that accompany them. However, compulsions only provide temporary relief from the discomfort caused by the intrusive thoughts, and ultimately are what keeps the person with OCD stuck in the OCD cycle (see diagram below).
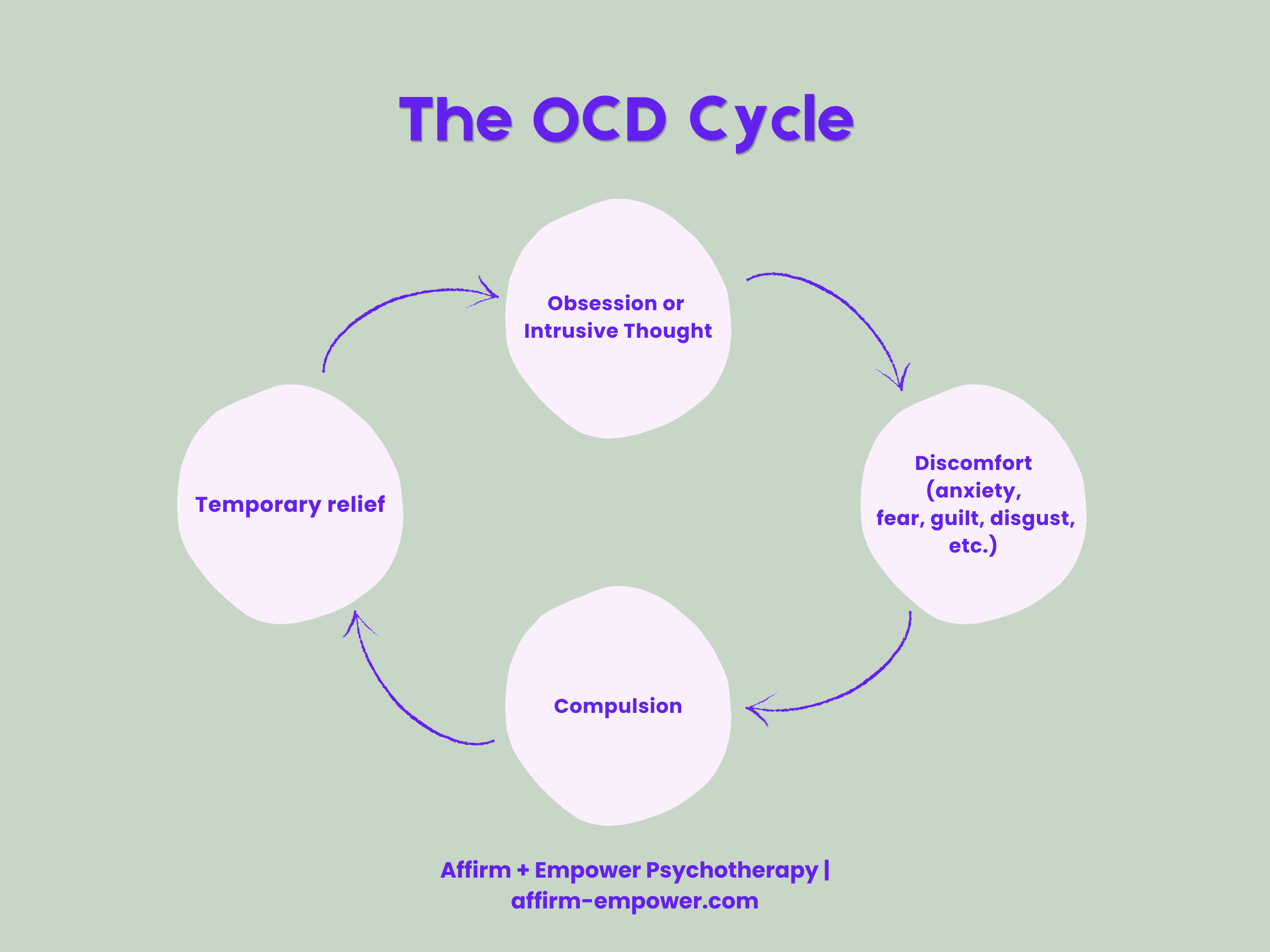
A diagram of the OCD cycle, illustrating how compulsions provide temporary relief but continue to fuel the obsessions.
The OCD cycle continues in this way, because a person learns by performing their compulsions (for example: avoiding feared people or activities, engaging in excessive handwashing or arranging of objects, etc.) that they will feel temporary relief from their intrusive thoughts and uncomfortable feelings. They learn: I have this uncomfortable thought, I then engage in the compulsion, and I feel better for a little bit. So next time I have that uncomfortable thought, I need to continue doing my compulsions in order to feel better.
Here’s an example of how the OCD cycle can play out for a person with harm-themed OCD:
The person experiences intrusive thoughts about purposefully or accidentally stabbing a family member.
The intrusive thoughts trigger feelings of anxiety, fear, and guilt—folks with this type of OCD typically feel so guilty for having these thoughts, it can feel as if thinking the thought is as bad as actually stabbing someone.
The person then avoids or refuses to use any knives that are not plastic, and will ask their spouse to do any cutting/chopping requiring a sharper knife.
The person with OCD then learns: I won’t stab anybody if I’m not using a sharp knife, therefore my compulsions help keep me and my loved ones safe.
The issue here is that the person continues to have the intense fear that they could hurt or stab someone. They never learn otherwise because their compulsions don’t provide them the opportunity.
How ERP Is Different
ERP is a highly structured therapy modality that involves exposing clients to feared stimuli (situations, places, people, etc.), while reducing (and eventually stopping) their engagement in compulsions. The idea is to put a client into a situation where they will feel discomfort and learn to sit with/move through the feelings without the use of compulsions. ERP is a gradual process, typically starting with exposures that the client feels will produce less discomfort and repeating each exposure several times until a significant reduction in discomfort is seen before moving on to a new exposure.
ERP is a very behavioral therapy; there is not a lot of analysis of the content of the obsessions, why they occur, or what they mean. This type of cognitive investigation is exactly why traditional talk therapy is not only unhelpful, but can actually make OCD worse. Instead, ERP’s goal is to disrupt the OCD cycle and create experiences where clients can experience new learning.
Why Does It Work So Well?
ERP is so incredibly effective because when done correctly, it creates that new learning through two things: habituation and expectancy violation. Habituation is the reduction of anxiety (or any other uncomfortable feeling) over time. When people with OCD engage in exposures, and especially when the exposures are repeated or engaged with over longer periods of time, they generally experience less and less discomfort (anxiety, fear, disgust, etc.) as time passes or as more exposures are completed. In other words, the emotional response to their intrusive thoughts and feared situations becomes less and less over time.
Expectancy violation occurs when a person expects to have a very high level of discomfort or anxiety in response to an exposure, and doesn’t. Their expectations were violated; they were shown that actually, this situation that they had feared so much turned out to not be so scary. Expectancy violation can be very powerful, especially for someone with OCD. It teaches them that they are capable of more than their OCD convinced them they were!
These concepts fall under Inhibitory Learning Theory: the idea that new learning through exposure can replace the old learning from the OCD cycle. Essentially, ERP teaches us that we are able to tolerate the intrusive thoughts and uncomfortable feelings without using compulsions.
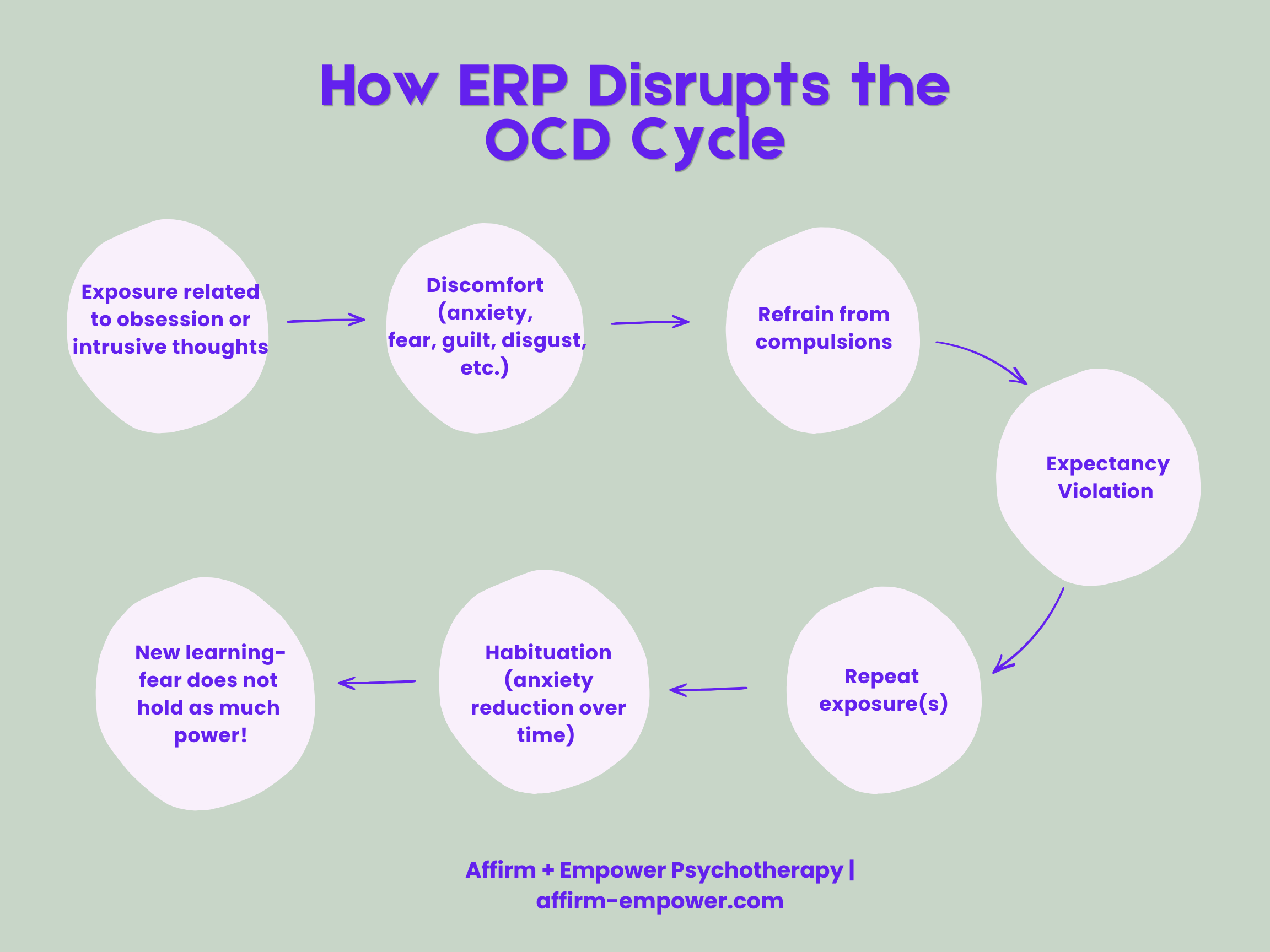
A diagram illustrating how ERP disrupts the ERP cycle and creates new learning!
Let’s revisit our harm-themed OCD example from above. Here is how this specific theme could be tackled with ERP:
The person with harm-themed OCD has said that cutting an apple with a knife while home alone would produce a discomfort level of around 6 out of 10 for them.
They then use a sharp paring knife to cut an apple in their kitchen while home alone.
The person experiences feelings of fear and intrusive thoughts around stabbing someone during the exposure, but they continue cutting the apple. During the exposure, they rate their discomfort as a 6.
After the exposure is finished, the client was able to see that they tolerated cutting the apple and experiencing the intrusive thoughts and feelings (and that they were able to do so without stabbing somebody—expectancy violation). They rate their distress afterward as a 4.
The client then repeats this exposure once per day for 3 more days, until they rate their distress during the exposure as a 2 or 3 (habituation). They then move on to another exposure that provokes slightly more discomfort—perhaps cutting an apple while their spouse is at home in another room.
ERP can quite literally be life-changing for people with OCD. It allows them to see how much more they are capable of; it opens doors to experience the things they had been missing out on due to avoidance or spending time engaging in compulsions. I love seeing clients’ faces light up when they tell me that their exposures were hard, but not as hard as they expected, or that once they started engaging in ERP, they didn’t realize how time consuming their compulsions really were. I love telling them how proud I am for engaging in this difficult but incredibly powerful work!
Sources:
Thampy M, Sudhir PM, Kumar A, et al. Inhibitory Learning-based Exposure Response Prevention Therapy in Obsessive-compulsive Disorder: A Development and Efficacy Trial Protocol. Indian Journal of Psychological Medicine. 2025 July 8; 48(1): 70-77.
Foa EB, Liebowitz MR, Kozak MJ, et al. Randomized, Placebo-Controlled Trial of Exposure and Ritual Prevention, Clomipramine, and Their Combination in the Treatment of Obsessive-Compulsive Disorder.Am J Psychiatry. 2005;162(1): 151-161.